A chronic disease that causes inflammatory “attacks” of the respiratory tract. The disease is very common, both in children and in young adults.
Lesson no. 14
Respiratory Emergencies
A chronic disease that causes inflammatory “attacks” of the respiratory tract. The disease is very common, both in children and in young adults.
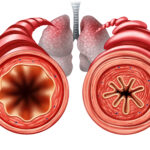
People with asthma suffer from bronchial hypersensitivity, which means that mild irritation will cause the release of a substance called histamine into the blood, which will lead to an excessive reaction.
Inflammation of the bronchial membranes causes the mucosal membranes to swell towards the inner space, which generates exaggerated secretion of mucus (essentially pus), and the combination of the swelling and mucus causes narrowing and/or obstruction of the bronchi. In addition, the body wants to protect the lungs so it causes a contraction of the muscles surrounding the bronchi. This narrowing process makes it difficult to exhale, which is usually a passive process.

A group of chronic obstructive diseases affecting the lungs, usually caused by prolonged smoking or long-term exposure to polluted air.
The disease is divided into two main types:
Chronic Bronchitis
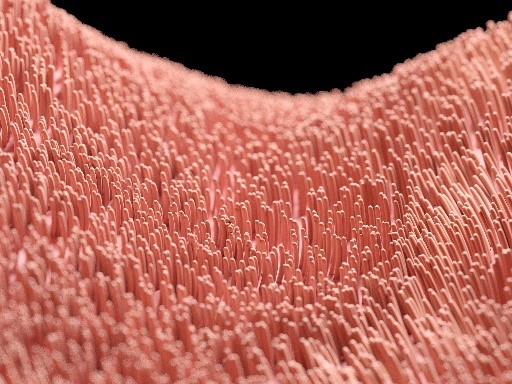
A disease in which the thin hairs (cilia) found in the airway are burnt as a result of hot smoke. As a result of the exposure to smoke, the inflammatory process secretes mucus that lines the walls of the airways. The bronchi become narrow which causes difficulty in breathing, especially in exhalation. Bronchitis is characterized by coughing periods that last for more than three months for no apparent reason, for at least two consecutive years.
As a result of the toxins in smoke, the walls of healthy alveoli are destroyed. Instead of small alveoli with a large surface area (a form that ensures quality gas exchange), we will have a few large alveoli with a small surface area. This will lower the efficiency of gas exchange. These patients usually appear to have a “barrel-like” thorax and abnormal thinness as a result of constant high respiratory effort.
Patients with these illnesses have difficulty breathing regularly, so when they call for help their normal condition has become worse and we’ll try to find the cause. This is usually due to another illness, such as pneumonia, the flu, etc.
Pay attention!
When a person is showing signs of respiratory distress, it is best to avoid long-answer questions, and aim for “yes” and “no” responses.
Over-ventilation of the lungs.
This condition is characterized by very rapid and superficial breathing, without any physical illness or injury. The condition is usually caused by high mental stress or anxiety. This will cause over-ventilation of the body. This means a decrease in carbon dioxide levels (increased exhalation causes a decrease in CO2 levels), which can cause a lowered state of respiratory stimulation (high CO2 levels trigger the breathing response) and even apnea.
It is important to note that as a result of over-ventilation, there is a change only in the carbon dioxide levels, while the oxygen levels in the body remain normal.
The only treatment is to calm the patient. This requires great effort in human relations and little medicine.
Hyperventilation should not show signs of significant shortness of breath such as cyanosis (blue skin) or other sounds when breathing (wheezing/crackling), so if we notice any more “serious” signs we will have to suspect something beyond hyperventilation.
Contrary to popular belief, the patient should not breathe into a bag as this may result in excess carbon dioxide, a dangerous condition in itself.

Choking is divided into two types:
Signs of complete obstruction choking: no speech, no cough, lack of breathing sounds, a red face from respiratory efforts, and later on, cyanosis (blue skin).
How to carry out the Heimlich maneuver: We’ll stand behind the patient. One hand should be made into a fist and the other hand wrapped around the patient, with both hands on the patient’s abdomen. Now a “J” motion should be made, pressed into the abdomen while raising the hands toward the chest, to contract the diaphragm toward the lungs and create positive pressure inside the lungs.

Signs of partial obstruction choking: coughing, difficulty breathing, sometimes wheezing while coughing.
Treatment

Drowning is defined as a life-threatening condition to a person/animal caused by water entering the lungs after submerging in water.
During drowning, water gets into the lungs and prevents proper gas flow. If water reaches the bronchial splitting point, a point called the carina, laryngospasm may occur – locking of the vocal cords.
The vocal cords are tissues horizontally located at the upper portion of the trachea. In the case of laryngospasm, they are completely closed and prevent entry and exit from the trachea.
We will distinguish between two types of drowning:
There are also differences in the type of water in which the drowning occurred:

In the case of hanging, we encounter a situation similar to choking as a result of a foreign object, since air cannot enter the lungs from the outside. Unlike choking, this blockage results from external pressure on the neck and trachea. In this case, the trachea is ‘squeezed’ and thus prevents air from entering the body. In addition, there are dangers such as breaking the neck and obstruction of the neck’s arteries leading blood to the brain.
For the most part, a person in a state of hanging will lose consciousness after about 15 seconds, and after a few minutes will suffer clinical death.
The responder’s place when arriving at the scene of a hanging may be critical and can save the person’s life if they arrive within minutes of the event, i.e. before brain death occurs. At the time of arrival, there is no way of knowing whether the hanging occurred in the last few minutes or not, so we will always treat the situation as if we arrived immediately after the hanging and that it is still possible to save the person.
Of course, not all hanging cases end in death, as there are accidents that cause the effect of hanging. For example, children playing with ropes.
Ways of identifying hanging injuries:
SIDS is a case where a healthy infant younger than a year has an unexpected and unexplained death that occurs during sleep. Unfortunately the cause of SIDS is unknown. Though there are many theories as to what causes this event, for example: bacterial infection or intra-fetal trauma, no theory has been proven in the slightest. That being said, we are aware of a number of critical risk factors that are speculated to be involved with SIDS:
Despite not knowing the direct cause of SIDS, there are several recommendations that came from research into the phenomenon that is supposed to help lower the chance of SIDS occurring.
All this and more. It is advisable to use a hard mattress for the baby, and a taut and tight sheet. To ensure the baby has a safe environment it is also recommended to distance pillows, dolls, and toys, to avoid any form of head protection or hats, and to distance all electrical products from the crib.
If the baby can co-sleep in the parents room but in his own bed will also reduce the risk of SIDS.
The use of a pacifier should be without the string attached to avoid any chance of suffocation.
The barking cough, known as stridor, is particularly common amongst children up to the age of five. The cause for this is that the respiratory tracts of children are significantly more sensitive than that of an adult. The source of the cough is a virus from a viral disease which can cause edemas and swelling around the vocal cords and in many cases lead to hoarseness.
It is important to make sure the child is in a vertical position, ie standing up. It is advisable to expose the child to cold air, for example by taking a short walk or opening the window. Using a cold humidifier can significantly improve the situation and help the breathing become easier. Lastly, you can treat the child with inhalations. In complex cases a doctor can give a prescription for a stronger medical inhalation that contains steroids.